Drowning in Alphabet Soup

 By Rebecca Oas, Ph.D. | October 30, 2015
By Rebecca Oas, Ph.D. | October 30, 2015
Why rapidly expanding acronyms are not the best prescription for global maternal health
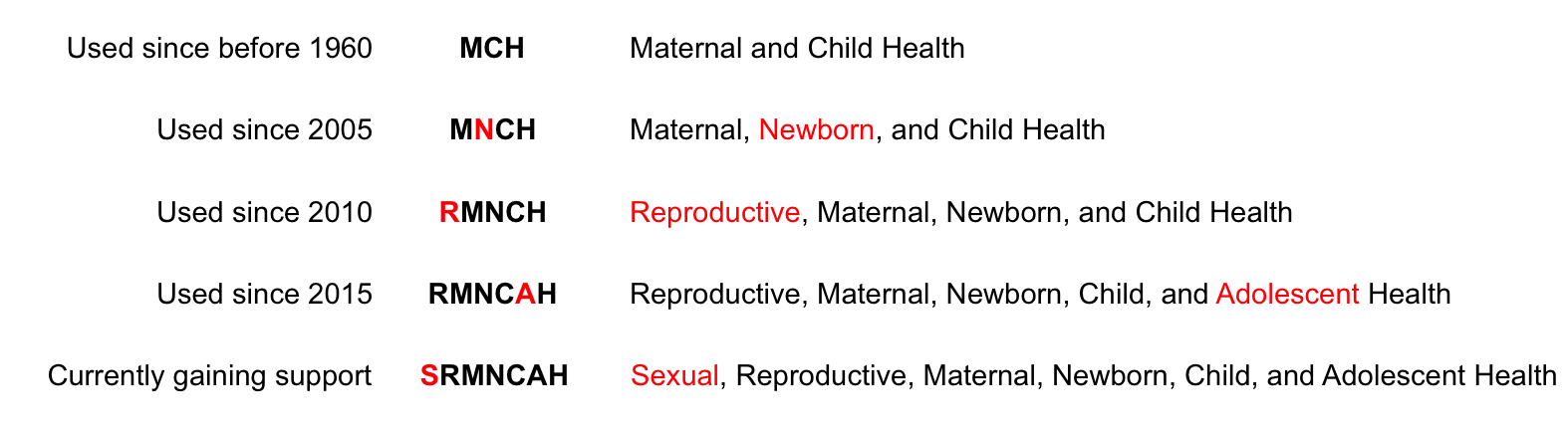
Earlier this year, the World Health Organization issued a report titled “Strategies toward ending preventable maternal mortality (EPMM)” Fittingly for a report with an acronym in its title, it included an entire page of abbreviations – 27 in all, for a document of less than 50 pages. One of the acronyms on the list was SRMNCAH, or “sexual, reproductive, maternal, newborn, child, and adolescent health.” While this particular formulation is of very recent vintage – as of this writing, it turns up less than 200 hits on Google – it is only the latest iteration of a rapidly expanding acronym focusing on maternal and child health:
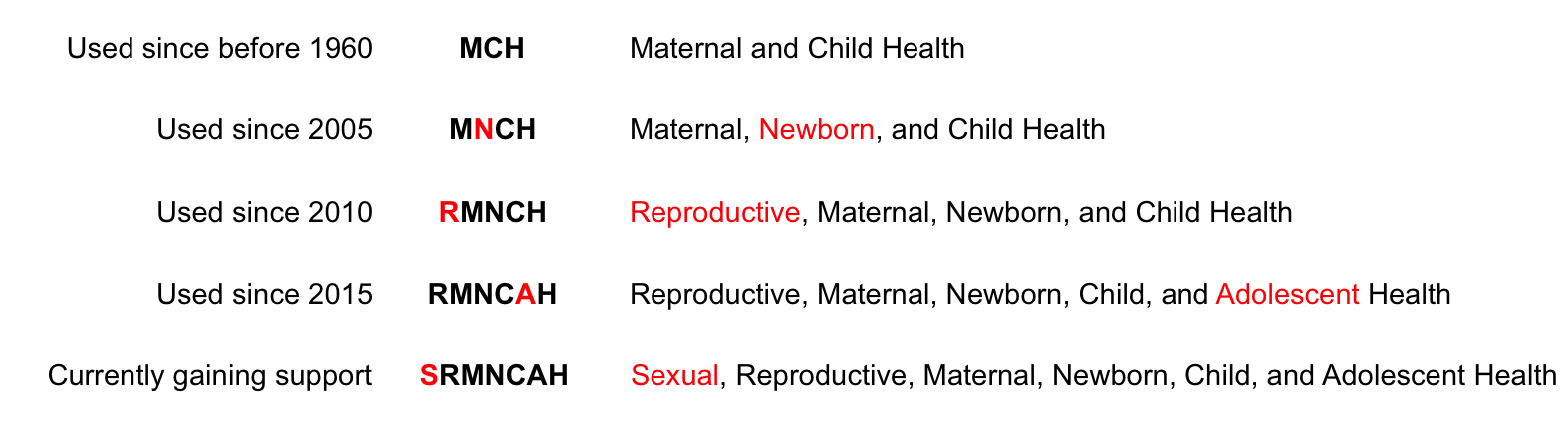
The second-to-last one, which only gained popularity this year, is RMNCAH (“reproductive, maternal, newborn, child, and adolescent health”) – that one has over 7,000 Google hits, for the sake of comparison.
Obviously, acronym expansion is not necessarily a bad thing – the inclusion of “newborn,” for instance, highlighted the fact that child mortality causes and rates differ between neonates and older children, and the remedies differ as well.
But the more letters and groups are added to the mix, the more you face the risk of mission creep, or perhaps more accurately, mission explosion. More focus areas mean more potential partners, but it also means more agendas pulling in different directions. Groups whose aim is to make childbirth safe find themselves yoked into partnerships with groups whose aim is to make it more rare, all vying for the same funding streams. For some organizations whose aim is to push a highly controversial social agenda in countries with high maternal mortality, attaching themselves the maternal health movement is a way to gain legitimacy as well as funding.
The argument in favor of adding letters to the sequence is always the same: it’s impossible achieve the stated goal without broadening one’s focus. But how broad is too broad?
In an article about Canada, which had become a global champion of maternal and child health under its previous conservative administration, Lancet editor Richard Horton wrote:
“The lesson of the past decade is surely that if you want to make progress for mothers and children, you need a broader compass—at the very least, a continuum of reproductive, maternal, newborn, and child health. The R of RMNCH had been dropped by a conservative government that, for example, saw the toll of over 20 million unsafe abortions as too “divisive” to discuss.”
The “R” was not so much “dropped” as “not added” by the Canadian government, which essentially earned the right to define its acronym by pledging massive support for the effort to improve women’s and children’s health through its Muskoka Initiative.
But as Horton admits, that “R” carries baggage. Canada’s government, which allows for abortion on demand within its borders, wasn’t necessarily opposed to discussing abortion-related mortality and morbidity; they just didn’t want to fund what Horton apparently sees as the only solution to the problem: widely accessible “safe” and legal abortion.
Not only does the “R” open the door to abortion provision and advocacy under the maternal and child health umbrella, it also brings in the family planning movement, whose motivations and methods are at best tangentially related to the interventions needed for pregnant women hoping for a good health outcome for both themselves and their children. While advocates of increased contraceptive use argue that better birth spacing reduces high-risk pregnancies, so does better nutrition, and we don’t yet see a second “N” added to the acronym. Moreover, some of the most vital contributions to improved maternal health are matters of water security, decent roads, and the building of modern hospitals and clinics. If family planning gets a seat at the maternal and child health table, why not urban planning?
But no sooner did the “R” get affixed than the advocacy turned to “A” for “adolescents.” After all, just as you can’t have maternal health without reproductive health, you can’t have reproductive health without making it available to the youngest potential reproducers. And “adolescent health” means you’ve just roped in all the “comprehensive sexuality education” advocates determined to undermine conservative social norms in developing countries by targeting the young people directly, through both formal and informal educational channels. Naturally, laws requiring parental notification and permission for minors to access “sexual and reproductive health services” would have to be struck down, which requires lobbying and pressure to be exerted in countries…wait, wasn’t this whole agenda somehow supposed to be about moms and babies?
The ink was barely dry on the “A” when rumblings began about adding an “S.” In February of this year, Katja Iversen of Women Deliver spoke after a panel at the “Global Strategy Stakeholders Meeting” for the UN initiative “Every Woman, Every Child” in New Delhi:
“Thank you…for reminding us about all the things we asked for and that we got. That was very good. So could I humbly ask for another thing? Could we…now we’re kind of talking about the continuum of care, “RMNCAH”…what about adding the “S”? That’s just a humble ask. The sexual and reproductive…Sexual and…reproductive, maternal, newborn, child, and adolescent health.”
The audience chuckled along with her as she stumbled over the increasingly unwieldy title.
This fall, “Every Woman, Every Child” announced their updated agenda, “The Global Strategy for Women’s, Children’s and Adolescents’ Health,” and countries and organizations made commitments to help further its goals. Notable among the political commitments was the Netherlands’ contribution, which included a promise to “prioritize sexual and reproductive health and rights” and “support 12 strategic civil society partnerships on sensitive issues concerning youth and sexual and reproductive rights, to the value of 290 million euros for the next 5 years.” To clarify the meaning of “sensitive issues,” we can look to the stated mission of the Danish-Dutch “Amplify Change” grantmaking apparatus. Via the Guardian:
“The fund will target groups that are working on often contentious issues, such as improving access to safe abortion or working to decriminalise it, protecting the sexual health of young people, or challenging female genital mutilation or discrimination on grounds of gender or sexual orientation.”
The UK also specifically committed to promote “comprehensive programming, which includes sensitive issues that others find difficult but where action saves and transforms lives, including safe abortion, comprehensive sexuality education, family planning for adolescents…”
Other groups pledging to support the “Every Woman, Every Child” agenda included abortion providers International Planned Parenthood Federation, Ipas, Marie Stopes International, and the Planned Parenthood Federation of America, as well as other organizations that aggressively lobby for increased access to abortion.
Circling back to the WHO document on ending preventable maternal mortality, we find a strategic plan that includes a call for a “rights-based approach” to ensure that high-quality care is accessible to all who need it. To further explain, it says:
“Treaty monitoring bodies have also linked elevated rates of maternal mortality to lack of comprehensive reproductive health services, restrictive abortion laws, unsafe or illegal abortion, adolescent childbearing, child and forced marriage, and inadequate access to contraceptives.”
Treaty monitoring bodies, whose observations carry no binding authority whatsoever, are notorious for “finding” things in treaties that are nowhere to be see in the text. They are also utterly unqualified to give medical advice – all the “links” described above have a massive confounding variable: poverty. Higher maternal mortality is linked to the poverty of a country and the region in which the country resides, and its resulting lack of high standards of health care, which is why there are multiple countries in Europe and Latin America with strict laws against abortion and excellent maternal health.
The WHO was among the first to adopt the “S” as suggested by Katja Iversen, and we can already see where that will lead us:
“All countries should increase efforts to reach vulnerable populations with high-quality primary and emergency SRMNCAH services. […] Vulnerable populations include: the urban and rural poor; adolescents; commercial sex workers; people who are marginalized; the socially excluded; lesbian, gay, bisexual, and transgender population…”
So now we’re providing maternal health services to gay men? So much for the WHO’s purported “guiding principle” to “protect and support the mother–baby dyad”…if they’re not tearing that dyad asunder by abortion, they’re ignoring it entirely in favor of campaigning on behalf of men who a) will never give birth, and b) will never father a child at all without renting eggs and a womb somewhere.
This movement has not only lost its sense of identity, it seems to have lost its mind. Guided by the principle of “you can’t do anything without everything,” it has become infested with special interest groups holding up the tragic image of a woman dying in childbirth to emotionally blackmail the world into supporting their wholly unrelated agenda.
Mothers and their children deserve better than that.
View online at: https://c-fam.org/turtle_bay/drowning-in-alphabet-soup/
© 2025 C-Fam (Center for Family & Human Rights).
Permission granted for unlimited use. Credit required.
www.c-fam.org