Saving Lives Without Leaving Survivors

 By Rebecca Oas, Ph.D. | August 25, 2017
By Rebecca Oas, Ph.D. | August 25, 2017
The United States Agency for International Development (USAID) recently released the latest progress report for its “Acting On the Call” initiative, which seeks to reduce maternal and child deaths in 24 priority countries (Burma was added as a 25th priority country in 2016).
The goal of the project is laudable: to save the lives of women and children, and when it was launched in 2014, the projection was that U.S.-funded interventions could save the lives of 15 million children and almost 600,000 women by 2020.
About a third of those 15 million children are not like the others: they are phantoms that do not exist now and will not exist in the future, by design. They exist only within statistical models, labeled by USAID as “child lives saved from demographic impact.” According to the original 2014 “Acting On the Call” report, “demographic impact” is defined as “the projected impact of family planning interventions on reducing the number of deaths due to fewer unintended pregnancies.”
Some children die before the age of five, many in the earliest stages of infancy. This happens for a variety of reasons, many of them preventable, and the rate at which this occurs is higher in poorer, less developed countries, including many of USAID’s priority countries. So, the logic goes, if family planning use increases in those countries, pregnancies and births will be averted. Some of those children would likely have died under the age of five. Therefore, by averting their existence, USAID will claim to have saved their lives.
It is not unreasonable to expect that “saving a life” should result in a living survivor. By characterizing these children as “lives saved” rather than “deaths averted” the “Acting On the Call” report is somewhat unusual — other analyses at least make a point of separating the two when the death is averted by averting the person’s entire existence. But even referring to these phantom children as “deaths averted” obscures important truths.
USAID’s estimates of child lives saved are generated by a statistical model that incorporates demographic information, child mortality data, and the rates of success of various health interventions. To calculate “lives saved from demographic impact,” the model applies the rate of child mortality to the number of projected pregnancies and births averted. In Afghanistan, for example, the under-five mortality rate in 2012 is estimated as 98 deaths per 1,000 births. The target mortality rate for 2020 is 54 deaths per 1,000 births. “Acting On the Call” estimates that between 2012 and 2020, 170,000 child lives can be “saved from demographic impact.” If we assume an average mortality rate of 76 child deaths per 1,000 births, averting 170,000 deaths would require averting about 2,237,000 births, of which over 92% would be expected to survive past the age of five. A look at all the priority countries reveals a similar trend:
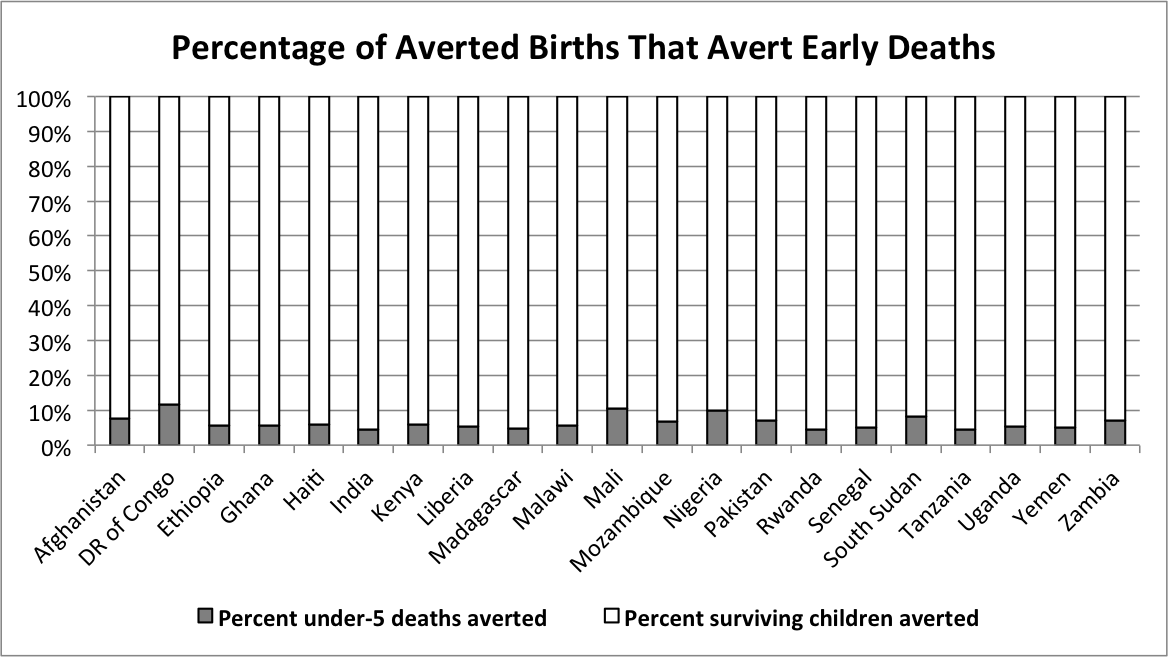
Taken together, averting the estimated roughly 5 million child deaths by “demographic impact” across the priority countries would require over 80 million averted births, of which some 94% would be expected to survive past the age of five. (This would require an even larger number of averted pregnancies, if we accept the 2012 estimate that 38% of unintended pregnancies worldwide result in a live birth.)

As cynical as it is to claim nonexistent children as “lives saved,” the problems with the “demographic impact” measurement go much further. Firstly, it’s an incredibly blinkered approach: if USAID wants to include hypothetical children in their analysis, they should include all of them, not just the minority estimated to die in early childhood. If, instead of “lives saved,” USAID decided to measure the number of children surviving over the age of five due to their interventions, the number of survivors would be dwarfed in each priority country by the number of hypothetical lives averted that would be expected to survive, but, thanks to USAID, were never conceived.

Secondly, lumping together the 10 million deaths averted by addressing childhood causes of death and the 5 million averted by “demographic impact” obscures the fact that these two measurements are in tension with each other. The former category works to drive down the child mortality rate (deaths per 1,000 births), while the other increases as the mortality rate increases. The more likely children are to die in a given setting, the more child lives one could claim to “save” by increasing contraceptive use. The reverse is true as well: the lower child mortality falls, the less effective contraception is at saving those hypothetical lives.
But when one considers the cost-benefit analysis for various interventions, it’s a lot cheaper to provide family planning to avert pregnancies than to provide for the full range of pregnancy-related, maternal, and child health care to ensure a healthy outcome for mother and child alike. If we’re willing to overlook the enormous amount of human capital the hypothetical 94% of averted births would bring to the world, the relatively low cost of averting the 6% of early deaths could arguably make family planning look like a “best buy” for global health and development, ahead of the other interventions USAID provides. That, of course, is the argument of family planning proponents, who would point out that the pregnancies and births being averted are unintended, and therefore more of a loss by their existence than by their nonexistence. But this case falls short in two respects: firstly, no less an authority than the World Bank concedes that children whose births are unintended tend to fare just as well in terms of health and education as their more intended counterparts. Secondly, cost or lack of access is not a major reason for contraceptive nonuse, even in less developed countries and regions.
Ending preventable child deaths is a worthy goal, and USAID is well positioned to ensure that more children survive past the age of five in their priority countries and drive down the mortality rate so that the tragedy of child death becomes a far more rare occurrence. But padding the numbers of lives saved with phantom dead children—and completely ignoring a far larger number of phantom surviving children—is not the way to achieve that goal. When a child dies too soon, it is because of disease or injury, not because he or she had the misfortune to be conceived and the bad luck to be born.
View online at: https://c-fam.org/turtle_bay/saving-lives-without-leaving-survivors/
© 2026 C-Fam (Center for Family & Human Rights).
Permission granted for unlimited use. Credit required.
www.c-fam.org