Event Highlights Divided Priorities in Global Maternal Health Agenda
WASHINGTON, DC, December 15 (C-Fam) Thirty years ago, experts and activists joined to put maternal health on the international aid agenda. A daylong event in Washington to celebrate 30 years of the Safe Motherhood Initiative last week revealed differences in priorities between the coalition’s Western activists and its African practitioners.
Deaths of women in childbirth were once a neglected issue—one panelist mentioned a 1985 Lancet article that asked, “Where’s the M in MCH [maternal and child health]?” The movement gained traction at international meetings such as the 1994 International Conference on Population and Development, and gained particular prominence in the 2000 Millennium Development Goals (MDGs), where improving maternal health was a goal unto itself.
Abortion advocates—including several of the pioneering members of the safe motherhood movement—have long injected controversy into what would otherwise seem an entirely benign effort. Scholars have noted that the maternal health movement contains two camps: those whose focus is on the provision of health care, and those whose expertise is in advocacy for “sexual and reproductive health,” including contraception, abortion, and “sexual rights” issues.
At the Wilson Center event, both groups were in evidence: the former represented by midwives from sub-Saharan Africa, and the latter by Ann Starrs, president of the pro-abortion Guttmacher Institute.
Address Malata, an expert in nursing and midwifery who also serves as a professor and university vice-chancellor in Malawi, spoke about the obstacles to improved maternal health in her region of Africa. Midwives are frequently recruited away from the profession to work in other, better-paying fields. Basic infrastructure and transportation are often lacking; Malata told the story of a woman who labored for 48 hours before an ambulance arrived to take her to a hospital, only to die on arrival.
In contrast, Starrs focused her presentation on the role of contraception in averting maternal deaths, arguing that for every dollar spent on family planning above the current level, $2.20 could be saved in maternal and child health costs. The Friday Fax asked how one could justify directing funds away from maternal health given the fact that women die from lack of access to basic health care, whereas little “unmet need” for family planning is attributed to lack of access. Starrs acknowledged that only about 5% of “unmet need” for family planning is access-related, but did not elaborate on the question of funding.
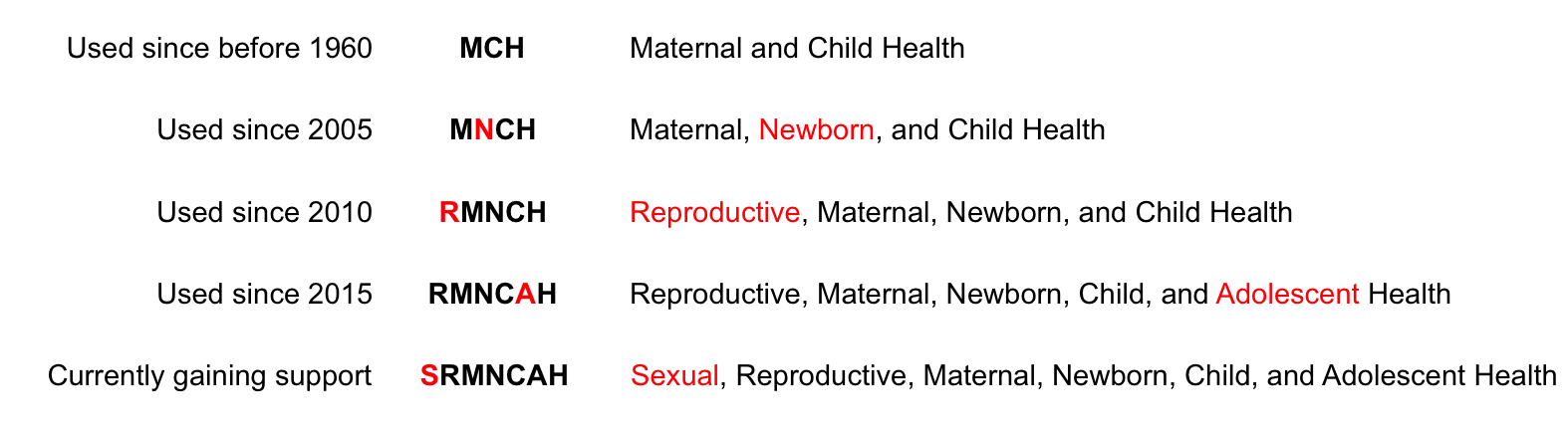
While progress has been made in reducing maternal mortality worldwide, it lags behind the targets established in the MDGs. In the ongoing Sustainable Development Goals (SDGs), maternal health has been demoted from one of five stand-alone goals to a sub-target under one of seventeen goals devoted to health in general. Similarly, the “M” that was once hard to find in “MCH” has now been buried within an expanded acronym SRMNCAH (sexual, reproductive, maternal, newborn, child, and adolescent health)—which Starrs jokingly referred to as “the sneeze.”
In the regions of the world where maternal outcomes are farthest behind—particularly sub-Saharan Africa—women die from lack of access to basic health care and skilled birth attendants, as well as broader gaps in utilities and infrastructure.
View online at: https://c-fam.org/friday_fax/event-highlights-divided-priorities-global-maternal-health-agenda/
© 2026 C-Fam (Center for Family & Human Rights).
Permission granted for unlimited use. Credit required.
www.c-fam.org